It’s been forever since I’ve done an eye update! Retirement is so much fun. I’m busier than
ever and I suppose it's a good thing that I'm not focused on my eyes.
But, this is a blog about my eyes and I write it in hopes that it can help someone. Here is an update.
Last summer, after a few false starts with adjustments and
fittings, I received my bioptics, or my Jordi glasses, as I call them. These
are a wonderful invention and they
 |
| Here I am enjoying Homecoming at the Citadel |
In November, I was honored to speak to the Lion’s Low Vision
Research Foundation (subject of earlier blog). I still want to do some kind of
volunteer work with them, but haven’t figured out how yet. Will work on that.
In January, I had a little scare. I went to my regular eye
doc, Dr. G., and she thought she saw what could have been a hemorrhage in my
left, the better eye. Hemorrhages in the macula are indicative of the wet form
of macular degeneration. A common remedy is laser treatment to stop the bleeding
and/or regular injections directly into the eye to prevent the growth of the
blood vessels that could cause the hemorrhage.
A friend who has macular degeneration gets these eye injections
regularly and I don’t know how he survives it. It is a fear for me, and I hope
I never have to have it done. I panicked
and was severely frightened that I might have to have a shot in the eye. However,
after my doc dilated my eyes and examined me some more, she determined that it
was an artifact of sorts and nothing to be concerned about.
 |
| Binoculars flipped up. |
 |
| Binoculars flipped down. |
During this visit, when we weren’t dealing with the
potential crisis of a hemorrhage, Dr. G. very ambivalently showed me the latest
and greatest glasses. She was hesitant because I had just spent money on the
bioptics and I don’t think she wanted to tempt me with the latest and greatest
gizmo to help patients with low vision. At the same time, she was very excited
about showing me what was going to be available. Well, I put the new ones on and was IN HEAVEN!
While my eyes were dilating, I wore the glasses and sat in the waiting room and
watched – read – the text stripe that crawls along the bottom of the TV screen
with the latest news. It was awesome! Dr. G. suggested that I come borrow the
glasses for a weekend. I told her it wasn’t necessary. If what they come up with is equal to these, I
want them! And the glasses are not horribly expensive – about 1200 dollars
compared to 2500. Hopefully all the bugs would be worked out by the time of the
next visit.
 In February, I went to my “new” retinologist at Wilmer. (My old doc, the one who I will always credit
with getting me on the road to rehab, moved his practice.) As is the protocol
with Hopkins, I was seen by several folks – students, residents, fellows,
technicians – before I saw her (or she saw me!). And they took a gazillion pictures. They did
a new test on me called an OCT. OCT means Ocular Coherence Tomography and it
measures the thickness of the macula. It wasn’t painful – more white lights and
sitting still. Not surprisingly, my results showed damage. It’s a fact
- I have abnormal eyes. This isn’t news to me. I just wish they weren’t so darned interesting
that everyone has to take a look!
In February, I went to my “new” retinologist at Wilmer. (My old doc, the one who I will always credit
with getting me on the road to rehab, moved his practice.) As is the protocol
with Hopkins, I was seen by several folks – students, residents, fellows,
technicians – before I saw her (or she saw me!). And they took a gazillion pictures. They did
a new test on me called an OCT. OCT means Ocular Coherence Tomography and it
measures the thickness of the macula. It wasn’t painful – more white lights and
sitting still. Not surprisingly, my results showed damage. It’s a fact
- I have abnormal eyes. This isn’t news to me. I just wish they weren’t so darned interesting
that everyone has to take a look! |
| This is a "normal" OCT. it shows about 10 different layers of the retinal. By measuring the various layers, the doctor can determine damage. |
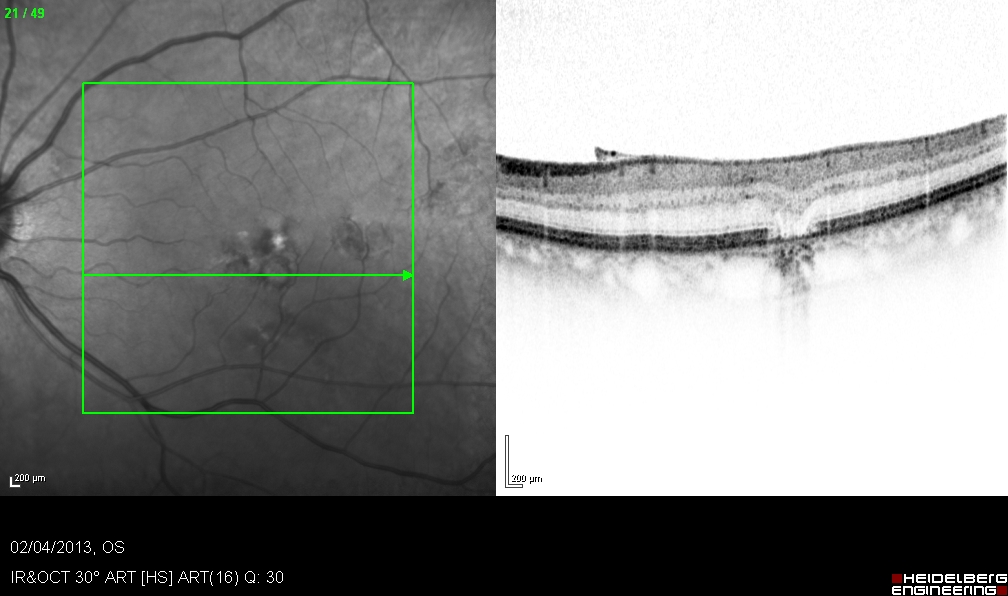 |
| One of my eyes. See the variation in the lowest layer. |
The good news is that my new retinologist says that my
disease may not progress at all, and I may not lose any more vision! This is
much better than a previous prognosis of “a 2 to 10 year window” before the
progression stops. Keep your fingers crossed.
In March, I returned to Dr’ G.’s office to be fitted for the
Ocutech Sight Scope, the new gizmo! These are regular glasses that have a flip
down binocular attached to them. The
binoculars are 2X power so the field of vision is significantly larger than my
bioptics. And they are lighter. The glasses arrived just in time for me to
attend, SEE, and enjoy a celebratory occasion for my nephew. I’ve had the
glasses for a week and a half, and, so far, I love them! And seeing street signs
is a breeze! I’m sure I’ll write more about these as I experiment with them. |
| Wearing the SightScopes |
So, what is it like for me to see? I’ve tried to come up
with a way to articulate it. If you have 20/20 eyes, or eyes that can be
corrected with glasses to 20/20, we don’t see the same way. When I go into a
supermarket or a big box store like Lowe’s, all of the stuff is overwhelming to
me. It’s like my brain can’t absorb it all and everything blurs together. I can
see a sea of red and white cans and I know that they are Campbell’s soup cans,
but they are blurred together. It’s too
much and I feel over- stimulated. I can’t read the signs in the aisles. It makes a difference if it is a store that
is familiar to me or if I am walking into a store where I have never been. If I know my way around, I can do just fine. The same is true with airports. I’m familiar with BWI and I feel comfortable
there, but a “new” airport makes me uneasy. I have to look around for
bathrooms, baggage claim and ground transportation. If the airport is busy, I
am even more uneasy. Again, too much stimulation and it’s hard work to absorb
it all.
I do know that when I am wearing my brand new glasses,
watching TV is very different. I can read the guide now, and the colors and
detail are clearer. I wonder what I have been missing! We have a small TV in
our bedroom, and from a distance, I can barely see anything. I use it as a radio.
I generally do what I want to do, but I have limitations,
and I have to accept them. Driving is the prime example. During daylight, in
familiar areas and non-busy times of the day, I’m ok. I panic sometimes when I'm out and it starts to get dark. I have to leave, I say, and that's hard. I’ve often thought of another career, but I’m
not sure I would trust myself. For example, I thought it would be fun to be a
pharmacy tech or a nurse. But, I can’t count on my accuracy. I just can’t have it both ways and that’s ok. There's plenty of life to enjoy!



















{kind=link}
{kind=link}
{kind=link}